What is a venous sinus? Like other parts of the body, the brain also has veins. Veins are vessels (small tubes) that are part of the circulatory system that drains blood from the tissue back to the heart. In the skull, the veins drain into the venous sinuses before going down to the veins in the neck. There are several venous sinuses throughout the brain cavity and are found between the outer covering of the brain (dura) and the skull. The venous sinuses also drain cerebrospinal fluidFluid that is made by specialized cells in the ventricles of the brain. Click the term to read more (CSFFluid that is made by specialized cells in the ventricles of the brain. Click the term to read more).
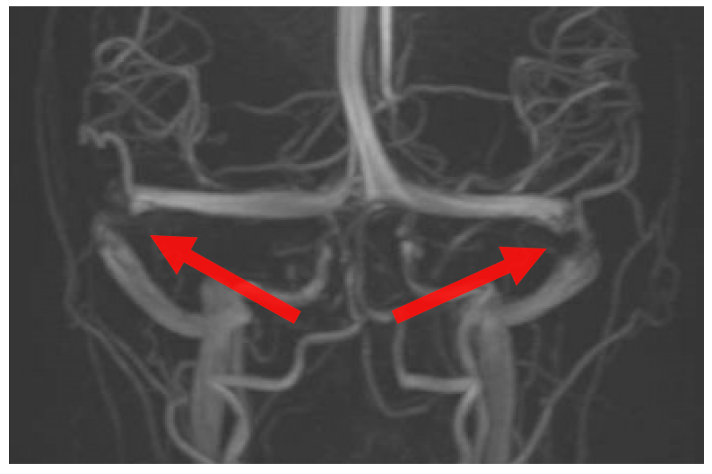
This image shows the veins and main sinuses draining the brain down to the veins of the neck. The red arrows point to stenosis of the transverse sinuses seen in IIH.
When the venous sinuses are narrowed or blocked, it can affect the pressure in the brain and the flow of blood and CSF throughout the brain. If the venous sinuses are narrowed (stenosed) it can cause an increased pressure in the brain and impaired drainage of cerebrospinal fluid and deoxygenated blood in the brain. This process will cause a person to experience debilitating headaches, visual changes, papilledemaSwelling of the optic nerve that carries visual signals from the eye to the brain. Click the term to read more, have an increased opening pressure on lumbar punctureA procedure where a needle is placed in the lower part of the spine (the lumbar spine) to access cerebrospinal fluid. Click the term to read more, and countless other symptoms. These described findings and many other symptoms are seen in IIH.
The reason why a venous sinus would become narrowed is not fully known. The current theory is there is an enlargement of the arachnoid villi in the brain. The arachnoid villi is what helps move CSF into the bloodstream. If these villi increase in size, it will decrease the size of the vessel1.
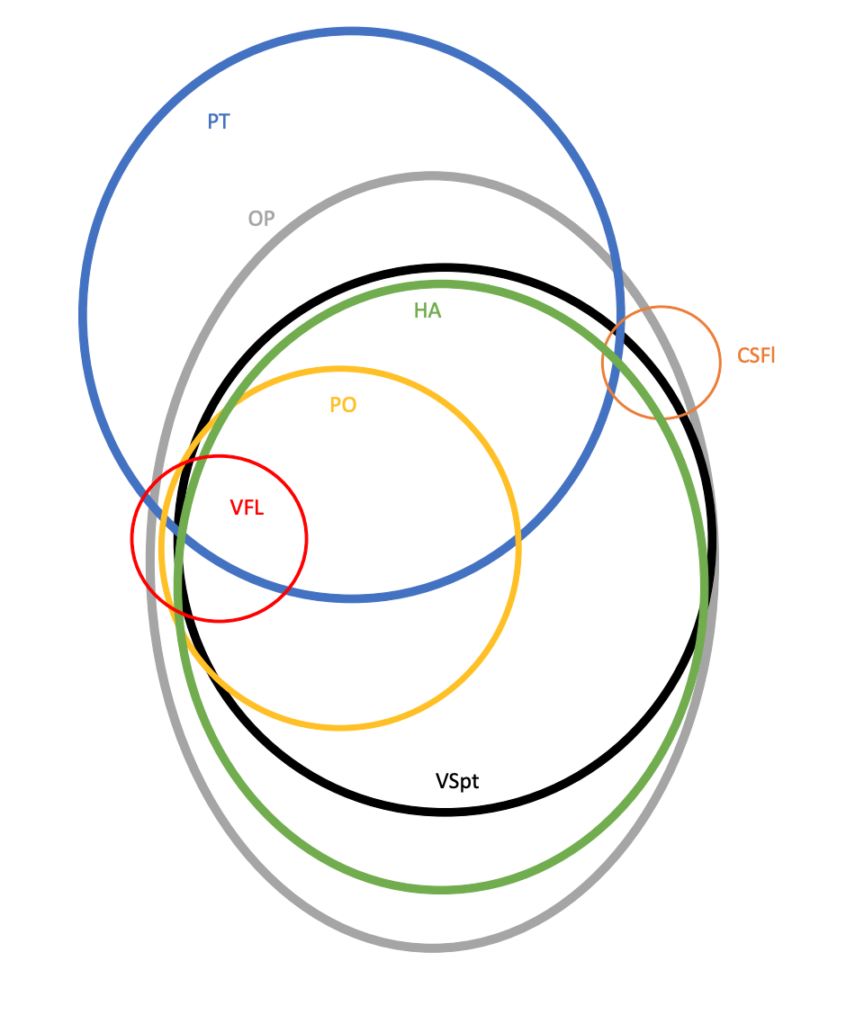
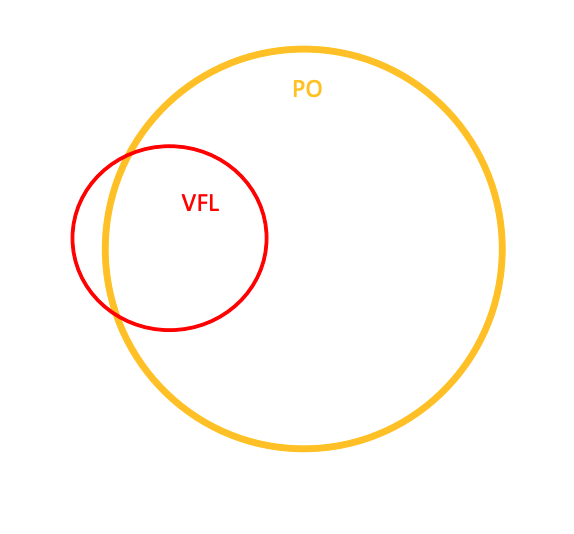
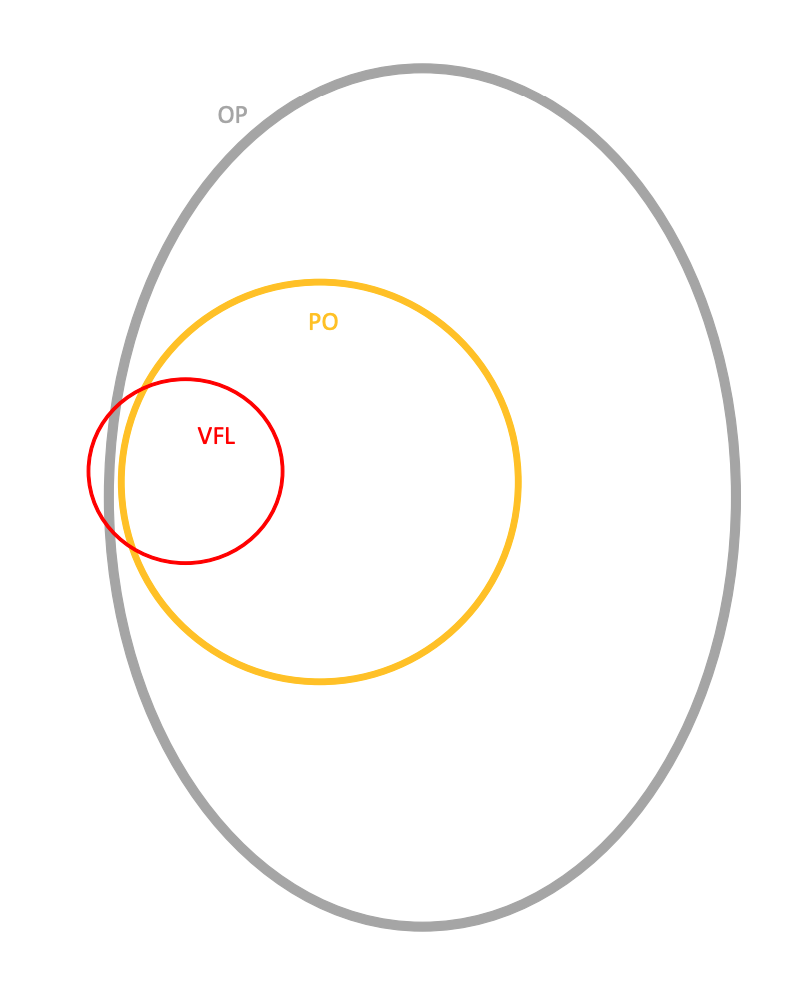
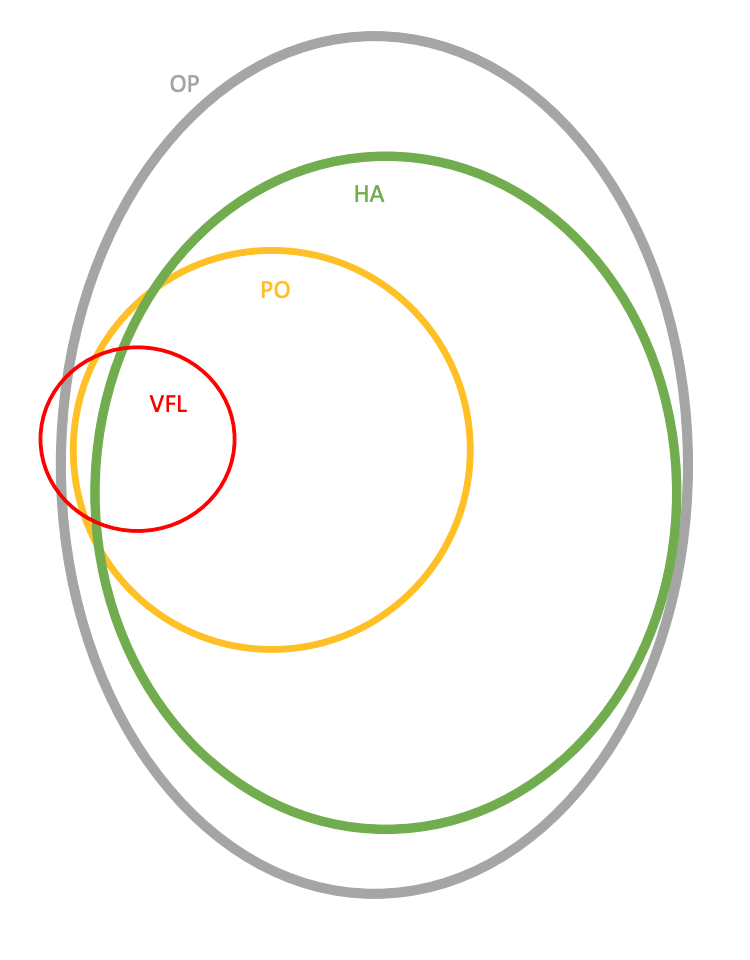
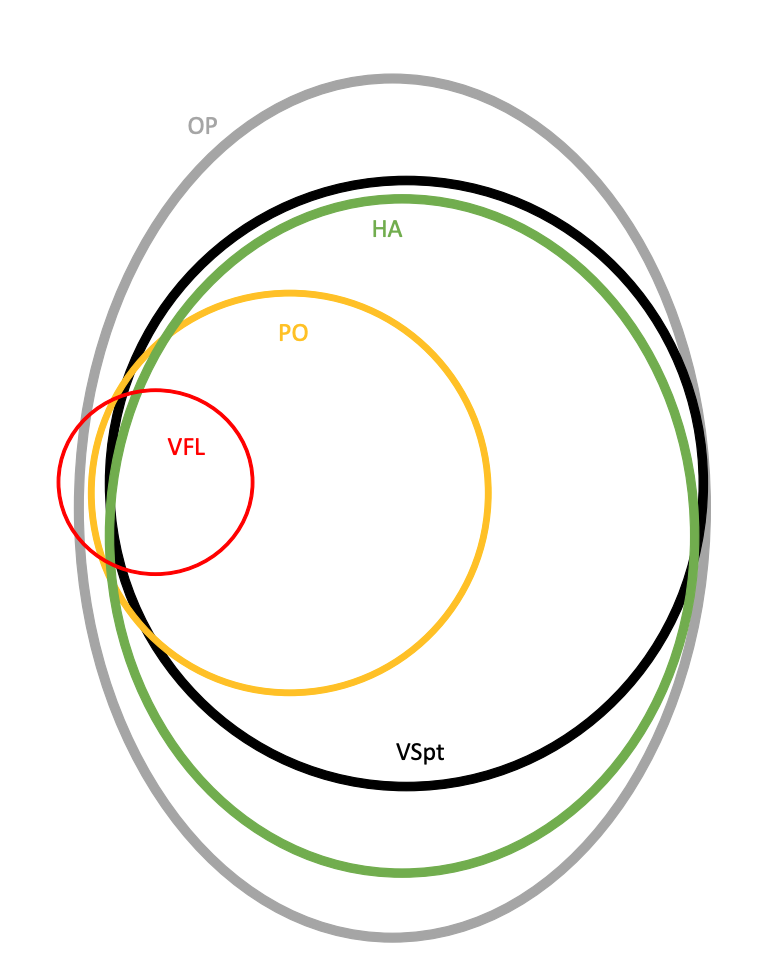
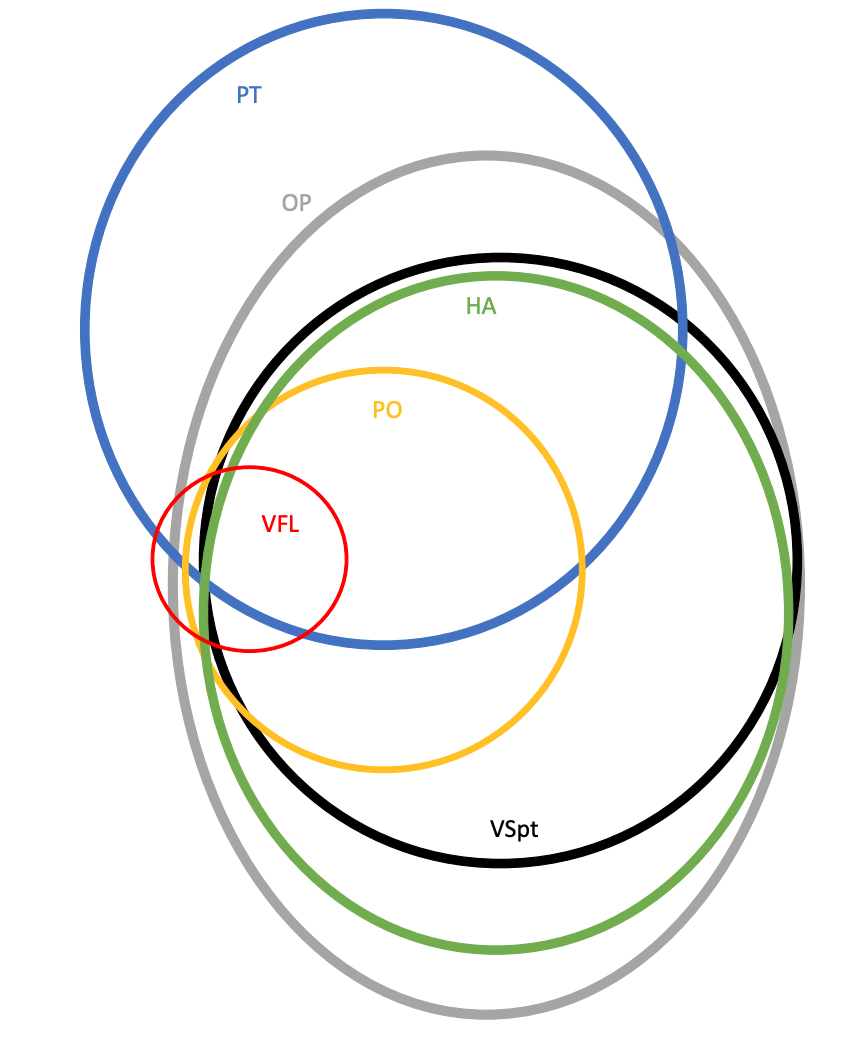
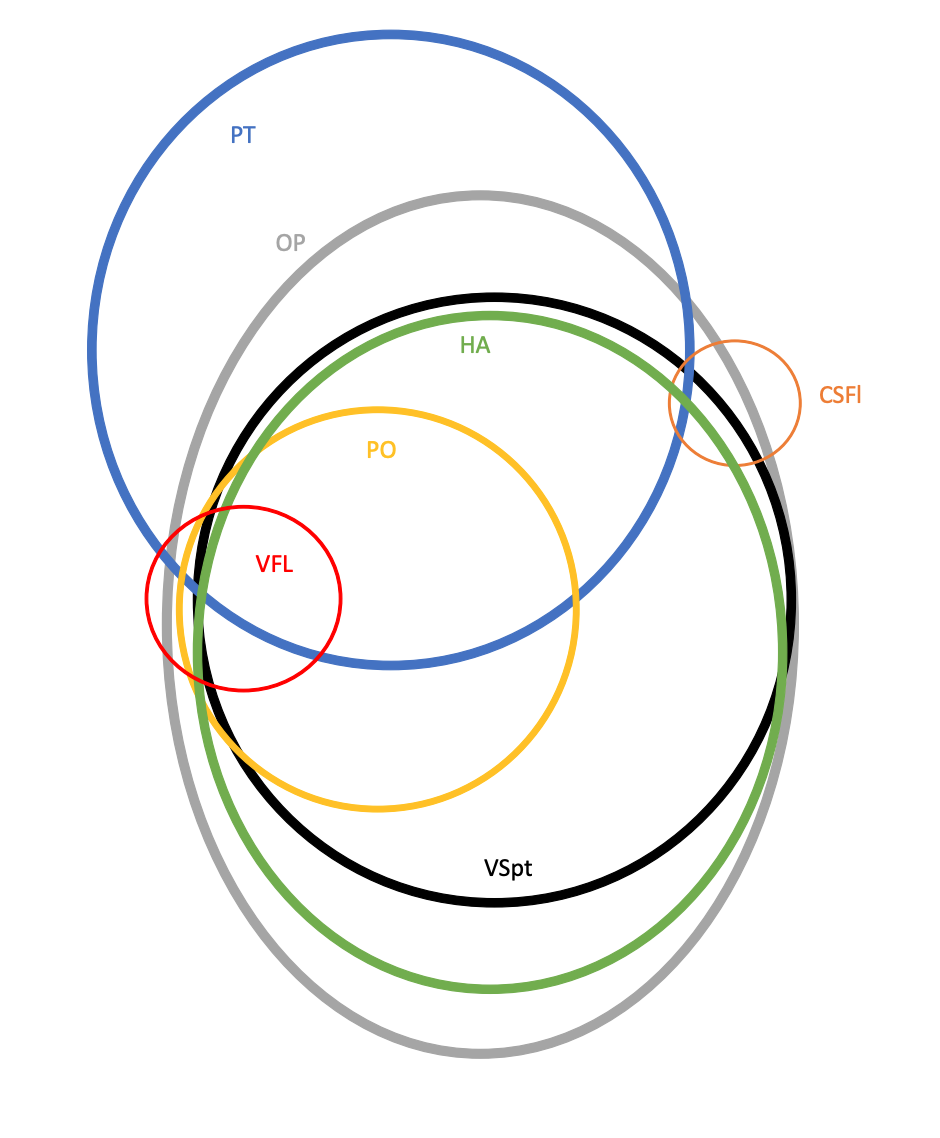
Using a Venn diagram, Dr. Pierre Gobin created a visual representation of how many common signs and symptoms of venous sinus stenosis are interrelated. The areas where the circles overlap shows a commonality between those two items. For example, a person IIH can have papilledema with visual field changes yet another person can have visual changes without papilledema.
Some people may have one, two, or a combination of described signs and symptoms but to receive a diagnosis IIH, the modified Dandy criteriaCriteria used for diagnosing patients with IIH. Click the term to read more is used:
- Signs and symptoms of increased pressure within the brain or papilledema without an identifiable cause
- Intracranial pressure is increased when measured in lateral decubitus position. This is obtained by performing a lumbar puncture and the opening pressure is measured at or greater than 25 cm of H20.
- The composition of cerebrospinal fluid is normal: clear appearance, WBC count 0-5 cells/µL, glucose >60% of serum glucose, and protein <45 mg/dL
- No evidence of hydrocephalus, tumor, infection, structural or vascular lesion
- Other conditions associated with increased intracranial pressure are ruled-out2