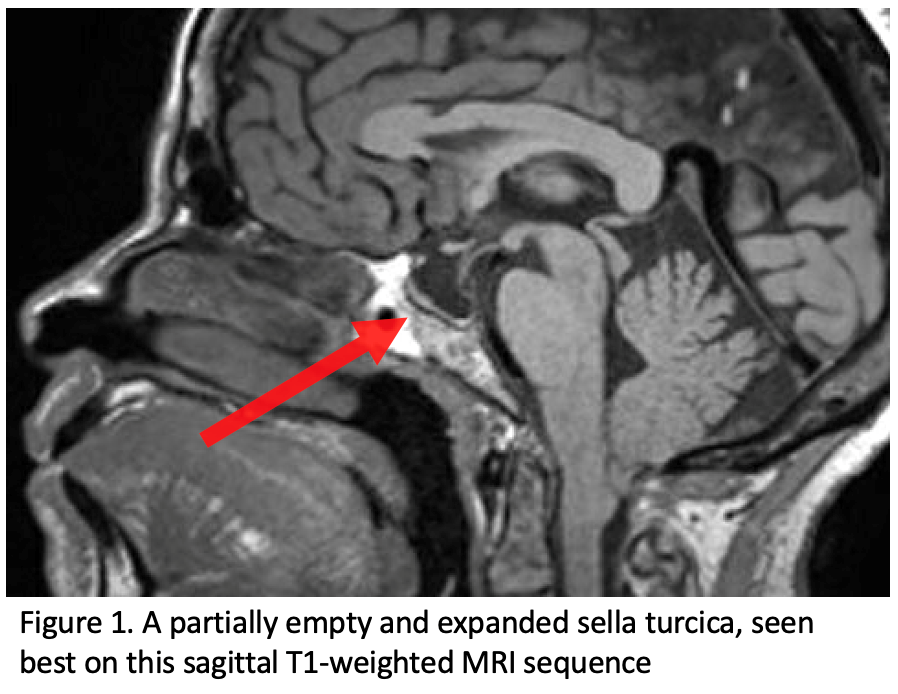
Patients with IIH should get imaging to rule out secondary causes of elevated intracranial pressure, including MR imaging and MR venographySimilar to an MRI – pictures are taken of the brain using magnets and radiofrequency. During the MRV though, additional pictures are taken to look… Click the term to read more of the brain. While imaging is performed to assess for secondary causes of intracranial hypertension, there are several imaging findings that can be seen with IIH. A partially empty sella turcica is a typical feature in the setting of IIH, which appears as a flattened pituitary glandAlso known as the “master gland” it is the area of the brain that manages and makes a large portion of your hormones. Click the term to read more within an expanded sella secondary to chronically increased ICPincreased intracranial pressure Click the term to read more (Fig 1).
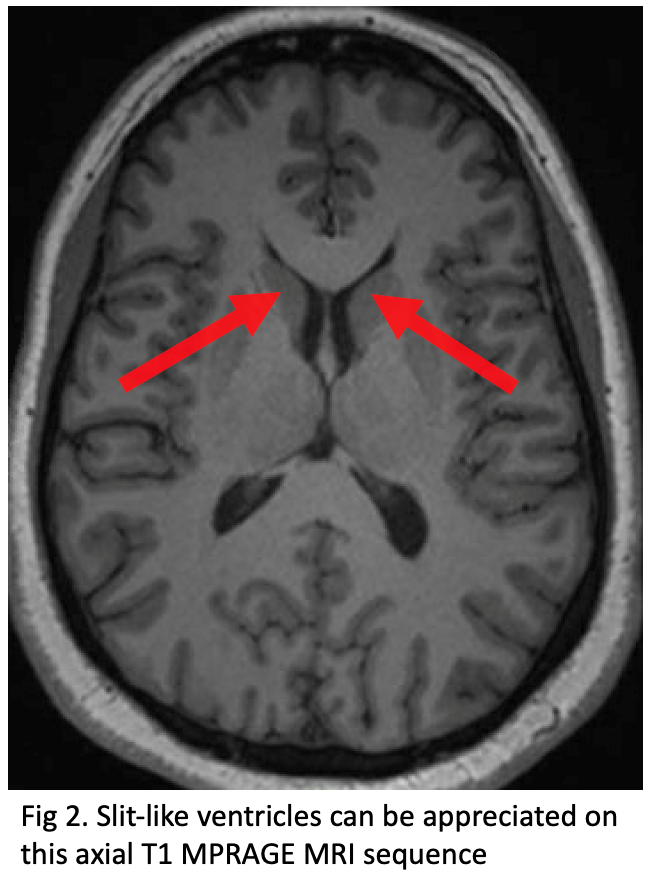
Additionally, slit-like or small compressed ventricles can be seen, typically involving the lateral ventricles (Fig 2).
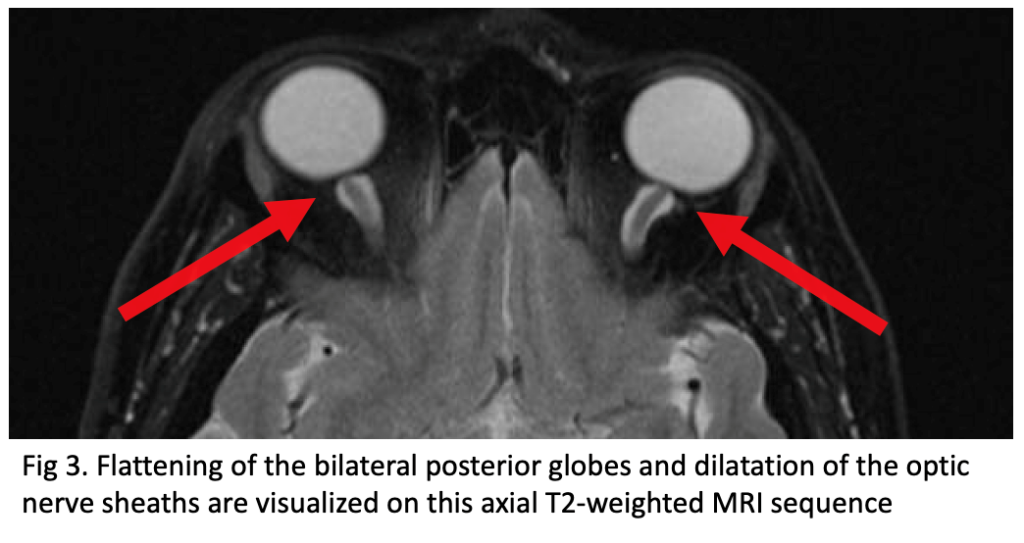
Another set of imaging findings in the setting of IIH is related to the orbits and includes posterior globe flattening, as well as dilatation of the optic nerve sheaths (Fig 3). The optic nerve sheath dilatation appears as increased CSFFluid that is made by specialized cells in the ventricles of the brain. Click the term to read more volume surrounding the intra-orbital optic nerve within the nerve sheath, which can also end up appearing tortuous.